




African Americans bear a much higher burden of cardiovascular health-related issues such as, poor blood sugar control, and blood pressure imbalances when compared with other racial groups. This often predisposes to poor kidney and cardiovascular function. The mechanisms for these disparities remain poorly understood, but likely include a combination of genetic, environmental, and socioeconomic factors.
Patients of African ancestry tend to suffer from more severe hypertension characterised by therapy resistance, greater vascular contractility and higher salt sensitivity, as well as a higher morbidity and mortality rate. For years, it has been known that patients of African descent respond better to Calcium channel blockers and diuretics than to ACE inhibitors and β-adrenergic blockers but it is not entirely clear why this is so. As a physician it is important to be able to personalise your therapy to the individual patient but some physicians object to the use of ancestry as a surrogate marker for therapeutic response. They argue that unique biomarkers should be identified and used to provide the best treatment plan in all cases.
However, Pharmacogenetic studies have not yet identified a reliable biomarker to predict therapeutic outcome. Consequently, ethno-geographic ancestry remains to be the most informative predictor of response to antihypertensive drugs.
There is an emerging view, however, that low nitric oxide and high creatine kinase may explain individual response to antihypertensive drugs. NO is an important vasodilator in the body which helps to reduce vascular resistance and subsequently, lower blood pressure. It has been found that Black patients generally have a lower level of NO and a high activity of the enzyme creatine kinase. Creatine kinase fuels calcium ATPase and governs calcium entry initiating vasoconstriction. Additionally, the higher creatine kinase may put a higher demand on creatine and induce a depletion of its precursor L-arginine which is also a precursor of NO. This NO deficiency is thought to lead to vascular endothelial dysfunction.
Decreased NO bioactivity can not only arise from impaired NO production, but also enhanced antioxidative pathways by glutathione. A recent study showed that homozygosity for the 4a polymorphism conferred a significantly increased risk of heart health issues before age 45 in blacks. Another important genetic determinant of NO synthesis and its oxidative inactivation is glucose-6-phosphate dehydrogenase (G6PD). A deficiency of G6PD is the most common enzymopathy globally, and it is particularly common in the US black population (15 percent prevalence). Recent work has shown, however, that G6PD is a key determinant of vascular function and that its deficiency can lead to impaired NO production and enhanced vascular oxidant stress.
Perhaps the most striking feature is that these health disparities are not seen in black communities within parts of Africa. This suggests a predominantly environmental influence rather than a genetic predisposition.
It is paramount, therefore, that precautionary measures are taken within the black community and a conscious effort is needed to change dietary patterns and lifestyle habits. For example, reducing sodium and glucose intake are likely to prevent a large percentage of these cardiovascular complications seen in Black communities.
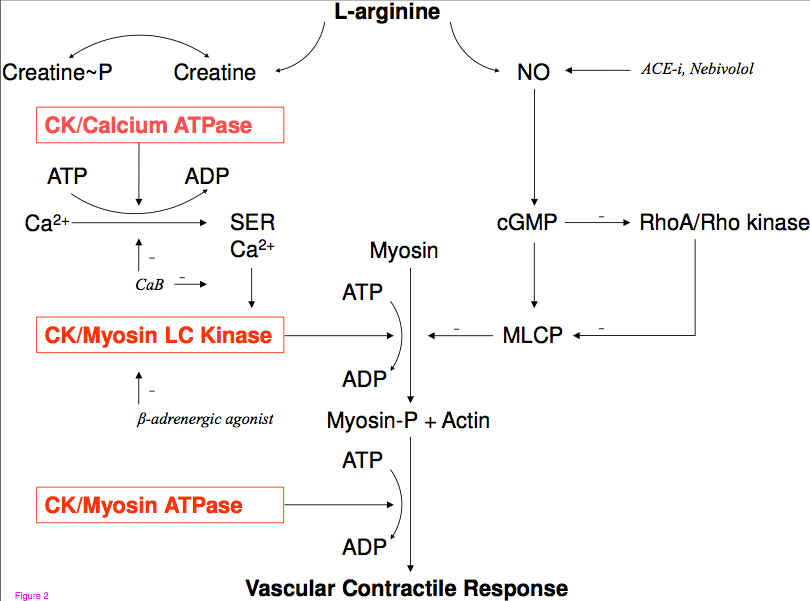
For medical students wishing to understand a bit more about the underlying biochemistry, I have included the figure above. In simple terms, L-arginine is the precursor for both Creatine and NO. Therefore, it is believed, that an increase in the enzyme creatine kinase, which directly phosphorylates creatine, puts a higher demand on creatine and this leads to less NO being produced. Furthermore, beta-adrenergic agonists normally inhibit CK and Myosin Light chain kinase (MLCK) so beta blockers will attenuate this favourable effect leading to greater levels of contractility in vascular smooth muscle and a higher total peripheral resistance (which subsequently raises blood pressure). In Europeans this pathway is not as important because there are sufficient levels of NO to inhibit CK and to activate protein kinase G and cause vasodilation through elevated cGMP, however, in the black population this pathway becomes a crucial one in maintaining blood pressure homeostasis because of the low basal levels of NO.